Muscle and Ligaments Sprain in Rhythmic Gymnastics
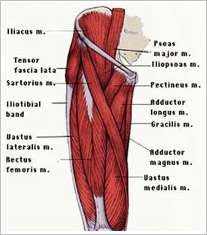
Flexibility is the main quality of a rhythmic gymnast and it can be developed by stretching exercises for the corresponding muscles and ligaments. That’s why injuries caused by the excessive stretching or sprain are fatal in rhythmic gymnastics. Hamstring and groin area muscles get injured very often in rhythmic gymnastics. Groin muscles consist of several muscles of medial side of the thigh, which have several layers (see the picture below). The main function of these muscles is hip adduction. Hamstring muscles on the back consist of semitendinous muscle, which is fastened to the medial part of the knee joint; biceps of the thigh, which is fastened to the lateral side of the knee joint; and semimembranosus muscle. The main function of these muscles is knee bending and hip extension.
So muscle pain can be caused not only by the sprain, but also by other reasons. Professor Francisco Bioska has his own classification of muscle pain:
Inner
Physiological (reversible changes of muscle fibers, without scar)
· Contracture (muscle contraction connected with the spasm)
· Delayed onset muscle soreness
Anatomical (reversible changes of muscle fibers, with scar)
- Sprain - I degree
- Muscle fibers rupture – II degree
- Muscle rupture – III degree
- Total Muscle Separation – IV degree
Outer
- Light bruise (I degree): local tissue reaction
- Bruise (II degree): muscle injury – hematoma
- Bad bruise (III degree): fiber breaking, total separation
Inner muscle pain is often met in rhythmic gymnastics. It’s important to distinguish anatomical pain from physiological one, as the treatment strategy depends on it.
Delayed onset muscle soreness
Delayed onset muscle soreness means reversible changes of muscle fibers without damage of conjunctive tissue, caused by muscle overload.
Clinical picture: pain appears some time or days after the long and extra load; not trained enough people suffer such pain, but professional sportsmen are not an exception. Pain bothers even in the quiescent state or when you touch the injured area.
Treatment: symptomatic, NSAIDs, pain is eased in a week. Differential diagnosis is held with the muscle stretch, it’s important to examine the mechanism of the pain occurrence.
Contracture
Muscle spasm is critical reversible changes of muscle fibers without damage of conjunctive tissue, caused by upsetting biochemical processes balance – myostatic tonus rise.
Clinical picture: sudden apparition, sportsman feels his/her muscle is shorter, pain even without touch, pain is not settled.
Treatment: there’s no need to treat in a special way, but this injury should alert sportsman, asбю perhaps, it is a signal of more serious injury. Usually it is caused by muscle fatigue. It’s better to correct the possible risk factors of injury, do stretch exercises, massage, continue training, if there’s no relapse.

Sprain, I degree
When the muscles are sprained, some muscle fibers suffer irreversible changes even till the necrosis state, but the elements of conjunctive tissues are not damaged. Ultrasonography finds microbreakage of the fibers.
Clinical picture: sudden apparition, during the peak of the load, pain while stretching, pain is settled while touching.
Treatment: rest, NSAIDs, muscle relaxant, relaxing massage, gradual continuation of training load after 4-5 days of rest (load intensity is defines by the pain occurrence). Total recovery comes when there’s no pain while stretching.
Sprain, II degree
Irreversible changes in the limited number of the muscle fibers with the minimal damage of conjunctive tissue elements.
Clinical picture: sudden apparition, sharp and piercing pain, spasm, pain while stretching, pain while touching, if the spasm is relieved.
Treatment: rest, Ultrasonography (twice), growth unducers, physiotherapy (cold during first 48 hours, magnet therapy, ultrasonic therapy, massage with ice, ТЕNS), eccentric training taking into account the indolence rules. Training load starts in the swimming pool. Ordinary training starts when the maximum load has been done in the swimming pool. Training in the group starts when exercises can be done by the gymnast in a high speed and without pain.
Muscle rupture, III degree
Multiple damage of muscle fibers and conjunctive tissues, intramuscular hematoma appears.
Clinical picture: sudden apparition, strong pain, loss of muscular agility, insignificant muscular weakness, spasm some hours after injury, topoalgia (local pain, but not pointlike till 4 cm2).
Treatment: in connection with the severity of injury and long recovery period, we point 3 levels of the treatment.
Level 1 (24-48 hours)
- primary treatment: cold, compression
- analgesics
- relaxant (neuromuscular blocking agent)
- general recovery program: diet, psychological training, keeping fit
- anti-inflammatory agent shouldn’t be taken
Level 2 (finishing – painless stretching)
- keeping feet
- exercises for stamina (35-40 min)
- electrotherapy
- TENS, supersonic rays
- relaxant (neuromuscular blocking agent)
- eccentric training taking into account the indolence rules
- rest for the injured muscle
- finishing – to increase the load for other muscles gradually
Level 3 (restart of training activity)
- gradual increase of the training load
- exercycle
- swimming pool
- restarting training (bearing in mind the criteria about muscle fibers rupture)
Train your muscles correctly and wear comfortable gymnastics leotards.
- See our gymnastics accesories.

01 Sep 2016 at 06:00
01 Sep 2016 at 06:00
01 Sep 2016 at 06:00
Like it? Tell your friends